Tomorrow's the big day! There's almost nothing more to do today except the bowel preparation, make a few phone calls, begin reading and viewing the
Integral Life Practice materials, nap, and get nervous.
I'm taking one last glance at my books about colorectal cancer to make sure I understand the information about surgery and recovery. I think I get it.
There will be abdominal shaving, an intravenous line set up while I'm still awake, a brief interview with the anaesthesiologist, a quick "see ya later" to my wife and son, a transfer to a narrow operating bed after being rolled on a stretcher into the operating room, possibly a quick hello with the surgeon and then, for me, lights out. I will probably get two types of anesthesia, a general and a spinal, the latter to help with postoperative pain control.
In the recovery room, I will be prodded into consciousness as the antidotes to the anesthesia are administered. Once the anaesthesiologist and recovery nurses are convinced I am breathing fully on my own, the endotracheal tube which was inserted into my mouth and throat to breathe for me during surgery will be removed. The recovery nurses will also monitor vitals to make sure there is no renewed internal bleeding.
When I am rolled back into the surgical ward, I will look something like a newly minted Borg specimen. There will be an oxygen mask, possibly a drain tube from the intestines, a nasogastric tube to assist with removal of gastric juices and gas, the intravenous line, a patient controlled analgesic device (PCA), a urinary catheter, and possibly, just possibly, a stoma with a temporary ileostomy device should the surgeon determine that my bowels will need additional time for the anastomosis to heal properly. All of that, plus the wound and dressings!
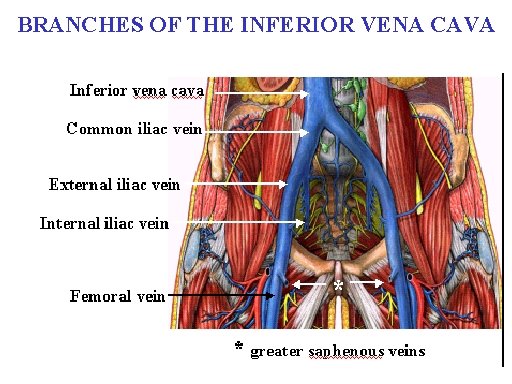
The urinary catheter, despite its distasteful aspect, is actually very important in helping nursing staff monitor urine output, thereby helping them adjust the intravenous according to how much fluid loss is occurring in the veins and arteries through a process called
third space loss. Three to 4 days later, the dangers associated with
third space loss diminish. It is at that time that I can look forward to removal of the urinary catheter, something my prostate cancer friends have warned me is quite unpleasant.
My body, especially my digestive system, will be in a state of shock, something technically called paralytic
ileus, when peristalsis stops in the intestines.
What this means for me is simply that the digestive system shuts down. So there will be no fluids given through ingestion until I have passed gas. Yes, that's right. I have to demonstrate that I can fart. When that happens, the nasogastric tube can be removed (another unpleasant but important milestone). It should be about the same time that the oxygen mask is also removed, around the 3rd or 4th day.
My duties are to administer pain medication using the PCA device whenever I will move in the bed, get out of bed to walk, or whenever the pain becomes too much. I will use an
incentive inspirometer to help me take regular (hourly) deep breaths, something important in preventing pneumonia.
I will also be walked regularly to help prevent clotting in the legs and the possibility of a pulmonary embollism. Even though I promised the radiation therapists in the adjacent cancer centre that I would visit on my fifth day, I now realize that occurs on a Saturday, so that trip will have to wait until Monday, my seventh day in hospital.
There will be regular dressing changes, another unpleasant necessity, removal of stitches in due time (the anastomosis will likely be held together with titanium metal staples), and finally a visit by the surgeon to tell me I can go home.
Apart from being nervous about pain, the various devices, and complications, the one aspect of all this which worries me is the possibility of post-operative confusion. Outbursts, out-of-character emotional responses (well, this might actually be a good thing; imagine me blessing everyone who comes by my bedside; that would certainly be out of character), delusions, etc. There's nothing that I can do beforehand to prepare for this except let me wife and children be forewarned. If I have confusion, I do hope it is minimal. I can hear it already from my friends, colleagues and family members - "Confusion? Too late!"

















%201.jpg)